

PROJECT OVERVIEW
Showcasing Industry Experts to Build Credibility as a Speaker
(Book Ghostwriting| Healthcare Supply Chain)
SNAPSHOT
The excerpt below was part of a book I ghostwrote for healthcare supply chain leaders.
GOAL
Position my client as a credible author—and a connector of experts—to support his speaking goals.
MY ROLE
Interviewer, researcher, and writer
APPROACH
I interviewed industry leaders from my client’s network, pulled out the most relevant insights for supply chain executives, and shaped them into clear, story-driven chapters that let the experts’ voices lead.
SUMMARY
The book showcased respected voices in the field, making my client the person who brings experts together rather than the “know-it-all” author. This
excerpted chapter highlights Intermountain Healthcare’s approach to purchased services, a major cost-saving challenge. It turns complex interviews into practical takeaways for readers, and builds credibility for my client as someone worth listening to on stage.
WRITING SAMPLE
Excerpt from A New Frontier: The Challenges and Opportunities in Purchased Services Contracting, a book on the health care supply chain that I ghostwrote.
Chapter 2: Driving ROI in Healthcare Supply Chains: Lessons from Intermountain Health
Intermountain is unusual in the industry in having never addressed supply-chain spend without including purchased services. When the IDN built its supply-chain organization, from day one, services were never out-of-scope.
“We didn’t start with med-surg, and then go to pharmacy, and then implants, and then decide to try and purchase services next,” says Joe Walsh, AVP, procurement at Intermountain. “We don’t ever really talk about just one sliver of our spend. We always talk about our total expenditures. We talk about our total spend management.” While acknowledging that an all-encompassing supplies and services spending approach isn’t necessarily the right pathway for everyone, he says Intermountain uses the same. processes, infrastructure, governance and talent to manage both the supply and purchased services sectors in spite of their inherent differences.
The Incentive to Pursue Purchased Services
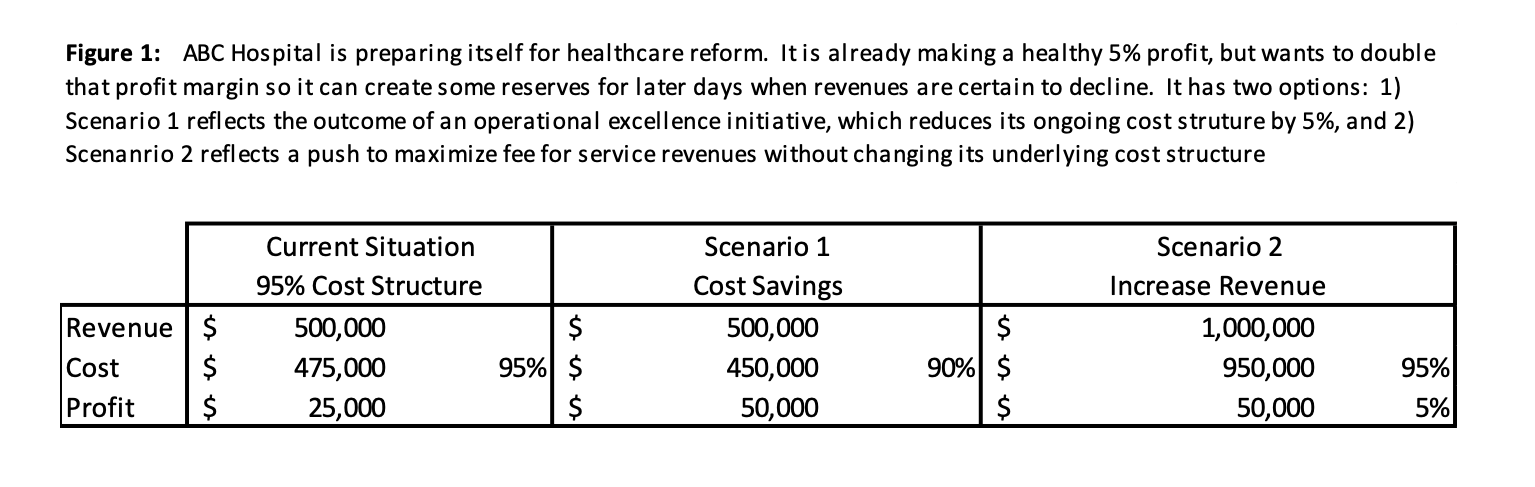
“First, it’s important to recognize the disproportionate impact of cost management relative to revenue,” says Walsh. “Every dollar saved on purchased services falls straight to the bottom line of an organization. This is significant. It often takes 15 – 20 times the amount of revenue to impact bottom line profitability to the same level as a cost savings initiative. [See Figure 1 for an example ]
“Second, we need to understand that not all costs are the same,” Walsh says. “There are fixed costs vs. variable costs and labor vs. non-labor expenses. The key is to understand what is addressable and controllable. Every dollar saved on supplies or services is a dollar that can continue to be used to fund the nurse at the bedside, where we need these important individuals.
“Finally, purchased services is a specific type of variable, controllable and addressable expense that is our next frontier of value,” Walsh continues. “Supplies and devices have been addressed by most hospital systems. For most organizations, purchased services are inherently more complex than other expense categories, which is why organizations avoid or defer the challenging work in these categories. However, the opportunity to create value for your organization is extraordinarily high in purchased services. With healthcare reform and the many revenue pressures our organizations face, our organizations will soon be asking us for solutions to dramatically lower our cost structures. Supply chain leaders have a responsibility to help their teams quickly develop capabilities in these areas.”
Walking Stakeholders Through the Math
Step one in developing those capabilities is earning the trust of service buyers. And that begins with conversations and tough questions. Walsh says one of the toughest questions is, “Why?” “Some people say, ‘[purchased services contracting] sounds like a nightmare,” he explains, “and they want to know, ‘why are we even talking about it?’ And the answer starts with that 20% you have to take out of your cost structure to survive on Medicare and Medicaid reimbursement rates,” he says. “So when people say, ‘Oh, let’s do more MRIs,’ we walk them through the math,” which is illustrated in Figure 1 above.
Scenario Two is the “do more MRIs” approach. Revenue has to increase astronomically to create only a 5% increase in profits.
“So if we’re trying to double our profit margin,” Walsh explains, referring to Figure 1, “all you need to do is drop your cost structure [Scenario One] by five points. That gets you an additional $25 million to the bottom line. But if you stay at 95% cost structure and 5% margin, and don’t change cost structure at all, you’ll need a half billion dollars to make that same impact. How many MRIs would you need annually to reach a half billion? It’s going to be a very high number.”
And purchased services go directly to the bottom line, Walsh explains. “Sometimes we end up getting such a reduction on our input cost that our net profit goes down because we get reimbursed at a lower level,” Walsh explains. “So cost is lower, but so is revenue, and we have a lower profit than previously. But purchased services is not tied to reimbursement, so dollar-for-dollar, savings drop to the bottom line. In that respect, services are not only as big as physician preference items, or bigger, but every dollar, 100% of it, drops to the bottom line.”
How Purchased Services is Different From Contracting for Supplies
“Purchased services is exponentially more challenging than other categories,” Walsh says, for a long list of reasons:
Buying Purchased Services Means Buying Expertise
Purchased services are typically highly differentiated (i.e., non-commoditized), which is a very different situation from supplies. “Supply categories such as office supplies and general medical supplies involve tangible, relatively undifferentiated products from a highly competitive supply base” Walsh says. “The service has largely been standardized as well so these categories have become differentiated primarily on price, which is the academic definition of commoditization.”
But purchased services are rarely commoditized, especially because you are contracting with a third party primarily for the skills, expertise, and/or the specific work product they can provide. “These are services, and service is almost never a commodity,” Walsh says, “because if you’re buying a service, you’re admitting you need expertise or you’re admitting that you need to hire someone to do something that you can’t do as well for yourself.”
In this respect, price is not the biggest question in determining the value of purchased services. We’ve seen this in other industries. The value of the expertise received and the time that’s freed up for a company or organization to pursue what it’s really good at – its core competencies – can become even more important considerations than price. “A hospital system may outsource its foodservice, payroll, HR benefits or environmental services functions, to free up resources to focus on even better patient care,” Walsh explains. “Outsourcing in that respect is the most mature and complex form of a purchased service.”
This dynamic is what’s driven the transition in most industries in previous decades toward outsourcing entire swaths of their operations – payroll, call centers, accounting, hiring, IT – to other companies, Walsh says. This trend toward outsourcing activities that fall outside an organization’s core competencies is one many health systems may find worth considering.
Demand for Purchased Services is Pulled vs. Pushed
Walsh says that demand for purchased services is pulled from the hospital, whereas demand for many medical supplies is pushed to hospitals by suppliers. Most hospitals are “product takers” in that they use and consume the products made available to them by product manufacturers. The supply of these products from the manufacturers shapes the use of these products for most hospitals. It’s also very rare for a product manufacturer to make a product to any one hospital’s specifications.
In contrast, purchased services are demand driven in that the demand for the services is pulled from the service providers by the hospital. For example, the demand for temporary nursing labor is created or “pulled” from the temp agencies as hospital census peaks. Just because a supplier makes a service available doesn’t mean a hospital is likely to need it or use it. Additionally, the hospitals often define the services they need very specifically and rarely take off-the-shelf service offerings.
The implications of this dynamic are significant. Forecasting necessary inventory levels for supplies is much more straightforward than forecasting demand for professional services. Previous purchases and consumption rates are poor predictors of future needs when it comes to most project-based services. Services are spread across a broad range of internal stakeholders, and when they need something—when the demand is created—then you go out and acquire the service.
For these reasons, pre-negotiating a services contract and presenting it to stakeholders for their future use is a losing strategy. “That’s just not how services are bought. It’s not how they’re required. First, stakeholders have a need and then we find a way to fill it, hence the demand-driven signal,” he says. “The purchase cycles are far more sporadic and unpredictable too.”
Purchased Services are Inherently More Complex
Even with relatively simple purchased services categories like training resources and temporary labor, services are inherently much more complicated to manage. And when you get into the categories that are even more complex, like legal and professional services, HR benefits and telecom, the plot thickens further. Like the simpler services categories, these haven’t been recently sourced, and they represent large spend and high savings potential, but there’s nothing simple about pursuing those savings. In doing so, supply chain teams must navigate stakeholder buy-in, where purchasing is strategic to the organization and has been non-transparent. There are more stakeholders to engage in the sourcing process and implementation is a project unto itself.
Even software is transforming into a service, thus the term “software as a service.” “You’re no longer buying the software, installing it, and using it internally,” Walsh says. “You’re actually buying a subscription and paying the company annually to keep it updated. That’s a service.” How is the software company going to support implementation? How often will they update? What responsibility does the company have for ensuring their program interfaces securely and effectively with other hospital databases and systems? These and many other questions have to be answered and those answers need to be organized to allow accurate comparisons between proposals.
It’s Difficult to Get a Handle on Cost Drivers with Purchased Services
When you’re dealing with a manufacturer, it’s with the maker of something tangible, so it’s easy to sit down and ask what percentage of the total finished product price is represented by the cost of the raw materials. It could be 60% to 80% for raw materials. The number doesn’t matter but the fact that there is a number does matter. Because now you can have an intelligent, transparent discussion about the suppliers’ cost drivers.
Walsh says this is part of developing a productive partnership with a manufacturer. “The goal isn’t to talk about the margin the manufacturer makes on the product,” he says. “Instead, I want to start talking about their cost drivers so we can work jointly on those and lower our costs together without shifting margin away.”
But you can’t do that with purchased services because, Walsh says, “the ‘raw materials’ are people. It’s a completely different type of category with a completely different set of dynamics. The business requirements are also dramatically different.”
Business Requirements with a Service are Often Much Harder to Define
What makes implants challenging, for example, is the relationship the physician depends on from the service provider. Walsh says they haven’t really been able to decouple those. “Ideally, we would like to get a definition of the service requirements our physicians need so these requirements can be implemented consistently, monitored and improved over time,” he says. “But because the product and service are so interconnected, it’s an almost impossible discussion because physicians can’t easily separate the products from the service, or the service from the products. That’s how tightly integrated the product and services are in this specific space. When service comes into the discussion, the complexity of the conversation increases.”
At this point the sourcing team needs to know the next set of questions so they can help end users define their service requirements. “We ask stakeholders thought-provoking questions that help them define the requirements,” Walsh says, “because otherwise they find it difficult to articulate.”
Using implants as an example, Walsh says the first thing his team brings to the conversation is acknowledgement of the physicians’ needs. “With our physicians, a procurement team member will sit down with them to collaboratively discuss total joints. We listen to their concerns and acknowledge that service is really important. We also explain our goals for pegging value and ask them to define the service elements that matter most to them. We may ask, ‘Is it the rep being available at 3:00 AM within 20 minutes of you calling them?’ We try to get the fullest and clearest picture possible of what the physician says the service should look like.’”
Their process of defining requirements is still evolving, but Walsh says, “In the next round we’ll get it, because it’s pretty straightforward. It’s just that physicians have never really been asked to think about and define what’s required beyond the product. Product and service were indistinct from one another. But we need to make those distinctions, because if you can’t define the service, there’s nothing to really build a fair agreement on.”
Providing another example of working to define requirements, Walsh describes the process they used working with their revenue cycle team on contracting with a third-party collection service. They began by asking stakeholders to describe what success looks like. The response was only a simple metric, that the collection rate should be X percent. Collection rate is important of course, but alone is insufficient to craft an agreement that’s best for the institution – and its patients. But procurement’s role at this point is only to prompt stakeholders to also think of other ways to measure value so those metrics can be captured and used in the evaluation process.
In their next step, Walsh says his team “asked a series of leading questions, including, ‘How do you ensure that the collection agency isn’t too aggressive with our patients?’ This is tough: How do you make sure you extend our culture and values to a third-party organization? We don’t want them to start over-collecting on our debt.”
The revenue cycle team agreed and listed other requirements, and Walsh’s team followed on with more questions: In what period of time do you need it collected? How many phone calls do you expect that to take? How long between the time you give them the account and the time they collect is acceptable to you?
“We had to ask them those questions,” Walsh says, “otherwise they couldn’t define the requirements, but once you ask them the right questions, they can give you the answer. They have it in their heads. They just need the right question to get it out.”
Intermountain Healthcare’s Journey to Purchased Services Proficiency
Supply chain’s original plan changed and evolved over time, but in retrospect followed five steps: Gain executive support, hire talent and establish structure, create the process, form governance councils, and track and use metrics.
With each subsequent step, organizational influence, scope and value increased, but it happened gradually: the supply chain team took two years to get process and governance, and decision rights in place.
The IDN’s purchased services total addressable spend is between $300 and $350 million. A sampling of categories includes: marketing services, temporary staffing, supply chain services, distribution services, and facility services.
Some categories change so dramatically from year-to-year, Walsh says, it’s almost not worth referring to last year’s number for projection purposes of any kind. “Consulting services is a good example,” he says. “What we plan to spend one year has nothing to do with what we spent the year before, because consulting is an absolute reflection of what we plan to do, not last year plus 5%.” Like many services spending categories, “consulting is always project-based.”
First Key Strategy: Get Executive Support
At Intermountain Healthcare, it started with a spend analysis, because without the data, getting executive support is a near-impossible endeavor.
Within his first month at Intermountain, Walsh led his team through a process of pulling and analyzing all expenditures. “What we found was that our number one spending category was consulting services, not physician preference items, and the biggest single payee on that list was a consulting firm used by the CFO. This particular consulting service was engaged and contracted without supply chain involvement, which was also the case with the majority of the consulting firms discovered in the spend analysis. The bottom line is I had to have a difficult conversation with the CFO, who is also our boss.”
Before presenting the problem to the CFO, Walsh and his team asked him an existential question: “Do you want us to just focus on supply chain process and projects or do you want us to be strategic?” Intermountain’s CFO wanted them to be strategic, and they began the discussion.
“We showed him the spend profile and then showed him that he was number one on our list of purchased services biggest expenditures. I said, ‘I can’t ask people to give up their autonomy with contracting services if we don’t set an example across our own finance function. We discussed the importance of ‘setting the tone at the top.’”
Walsh is grateful his CFO was so overwhelmingly supportive. And he says that without buy-in from senior leadership, a purchased services initiative is not likely to survive and it’s not a good use of resources. “If your hospital system execs don’t truly view supply chain as strategic and only view you as a pathway to contracts, then don’t invest the time. No hospital system will survive without making a meaningful impact to its cost structure and it’s our jobs as supply chain leaders to help make this connection for our senior leaders.”
Sending the “5% Letter”
The CFO demonstrated his support for purchased services in two important ways. First, he issued a letter to all functional VPs throughout the organization clarifying the expectation that the supply chain should be engaged for consulting services and other forms of purchased services.
Additionally, the CFO embraced the concept of sending out a letter to the majority of the current professional services organizations (which were not contracted through the supply chain). This letter clarified the supply chain’s role in extensions and additional services between their organization and Intermountain Healthcare. The letter also asked each supplier to submit ideas to the supply chain (and the functional business lead), which would reduce the cost structure on existing services by 5%.
“This was in 2008 and 2009,” Walsh says, “so these were hard times. We didn’t want to say, ‘Just give us 5% because we deserve it.’ Instead, we said, ‘The financial crisis has created unprecedented uncertainty and we need to explore ways to sustainably address our cost structure. We are targeting a 5% cost reduction in discretionary expenses. While we are willing to accept a price concession, this is not our expectation. We would like your ideas on how we can reduce our mutual cost structure so comparable services can be provided at a lower rate,’ Or said another way, how does Intermountain Healthcare help you reduce your cost to serve?’
The letter went out to all current suppliers with whom supply chain had not previously interacted, including all the vendors that were “sacred cows:” insurance companies, finance consultants, HR benefits providers, auditors, call center services, software companies and many others.
“Our internal stakeholders were understandably anxious we were going to damage their relationships with their partners.” Walsh says. “95% of the suppliers met the challenge and provided us with great ideas with practical implementation pathways. In fact, the total cost savings achieved with the targeted suppliers was 12.5% and we didn’t damage a single relationship with a supplier or stakeholder. In fact, this gave us an important foothold with many of our ‘new’ stakeholders going forward. In some ways, the ‘5% letter initiative’ was a very effective method for establishing trust with stakeholders and extending the supply chain’s influence into purchased services.”
Step Two in the Journey: Talent and Structure
In 2008, Procurement was trying to apply the infrastructure it developed to support the products/supplies side to the intangible purchased services. While some things ported over, like the sourcing process, others, like tactics, tools, and contract templates, needed to be dramatically different.
“People who become very proficient at total joints or buying something that has inventory implications are usually not the same people who are really good at buying software,” Walsh says. They needed specialization among their staff.
He says his team has been very fortunate to be able to hire people to tackle purchased services. That good fortune comes thanks in part to a smart strategy: Walsh never asks for a resource. Instead, he makes an offer, a commitment to their CFO that procurement will take $1.5 million out of the system’s cost structure every year for every MBA that his team is allowed to hire. But “MBA” doesn’t mean “freshly minted MBA.” It means “qualified person who actually knows how to do supply chain.” Intermountain compensates competitively, and the system gets an estimated $1.5 million back for every year they have that person.
When the CFO asks Walsh, “How many resources do you want to hire?” He responds, “How much do you want to save?” In institutions where savings don’t persuade leaders that hiring the right talent is worth it, “it’s probably time to go back to the ‘Gaining Executive Support’ phase,” he says. They need to recognize value can only be created with the right team members,” he says. “It’s worked at Intermountain. We’ve invested in competency development and have added resources responsibly– and we don’t take for granted the opportunity. Our stakeholders embrace this disproportionate investment because we ensure the stakeholders receive 100% of the credit for the value created and they get the spotlight for the success.”
Organizational Structure
Procurement is comprised of Solutions, Sourcing, Purchasing and Contract Management, and there’s a dotted-line relationship with Accounts Payable and Legal. There are 31 team members in the Sourcing team, which is responsible for the supplier selection process, contracting process, and category management process for more than $1.5 billion in annual expenditures. Walsh says, “Previously, we were asking the Sourcing team to take on too much in that we asked them to manage expense categories, stakeholder relationships, and supplier relationships. We had to dramatically simplify the roles in Procurement. Therefore, we created a Solutions team to manage the stakeholder and supplier relationships so Sourcing can focus their attention on our expense categories.”
Sourcing team members are organized around three main spend areas or “pillars” (software and services, equipment and maintenance, and products). This allows each team to develop highly specialized expertise for specific types of projects, such as purchased services. Sourcing team members have a diversity of experience – supply chain, nurses, doctors, IT, etc. The majority of employees are masters prepared.
Specialization Has Driven Efficiencies and Effectiveness
Sourcing deploys people based on their knowledge and experience. “Taking someone who does implants and then charging them with the task of doing a mega software deal doesn’t work,” Walsh says. “You don’t want those to be the same people – those deals require totally different skill sets. The processes are very similar, but the skill sets are dramatically different. The way you work with customers is different. The negotiation is different. The value levels are different. The tactics are different.”
Categories that fall under the software and services pillar have a lot of purchasing features in common: Strategies, contracts and tactics are very similar. But software and services is dramatically different from products and dramatically different from equipment and maintenance. Walsh’s team uses completely different strategies in the three different pillars. Two years ago, in recognition of these differences, they restructured people and gave them job specialization and doubled productivity while maintaining the highest service levels with stakeholders, he says.
The software and services team supports IT, financial, and clinical software, and it also supports all other services – except marketing, legal and construction. It’s made up of four people who manage $125 million in software/IT sourcing and $240 million in services.
On the products team, six people manage a portfolio of $700 million, including 16 categories and 196 sub-categories. They support clinical programs sourcing and contracting – clinical commodities, implants and pharmacy, and non-clinical products sourcing – food, linen and environmental services.
The equipment and maintenance team manages a $185 million annual capital plan. They support capital equipment evaluations and roadmap, construction and facilities sourcing, asset lifecycle management, equipment planning, value optimization team, the processing program and custom packs program.
Walsh says that all but one of the people on the three teams have their MBAs and they all have significant experience in the field they’re supporting, usually 10 years or more. The majority are CPSM certified from the Institute of Supply Management. “The MBA is so important,” he says, “because these teams are navigating physicians and senior leaders internally and very sophisticated suppliers externally. They have to understand the complexities of supply markets. We don’t want our folks going in and trying to negotiate with leverage alone. We think that’s very amateurish to just say, ‘We’re big, we’re important, so give us a better price.’ I’d much rather actually work with suppliers in a collaborative manner and figure out how to take cost out of our mutual supply chain.”
Specialist Team Handles the Tactical Work
Intermountain Healthcare manages 2500 contracts across 150 categories of expenses. The sourcing team creates or touches approximately 1,000 contracts per year. The activities needed to support each of these contracts vary dramatically. For example, the sourcing department facilitated 150 comprehensive sourcing projects in 2014, which led to 200 contracts. The team also has to support “service requests,” which include contract amendments, contract extensions, contract terminations, local contracts, and less complex sourcing events. In 2014, there were 800 contracts impacted by “service requests.”
“We quickly learned that it made financial and operational sense to invest in a team of sourcing specialists, dedicated to service requests,” he says. The sourcing specialist team is a combination of permanent employees and temporary resources, which allows the capacity to scale up and down with the variable demands of the service requests. This team delivers enables us to deliver an extraordinary volume of high-quality work for our stakeholders in a cost effective manner. The sourcing specialists benefit from career development as we lean on this team to build a strong bench of talent for future sourcing manager roles. The sourcing specialist team ultimately enables our highly qualified sourcing managers to concentrate their efforts on our most complex sourcing projects.”
Step Three in the Journey: Creating the Process
Process is really important, Walsh says. “Everyone has to be doing things the same way, especially when you’re growing.” Intermountain Healthcare’s sourcing methodology is the same for products as it is for purchased services, but there are some important points of customization.
Category-Specific Approaches
Products are selected based on identifiable product attributes and/or specifications. Purchased services are selected based on the service provider’s capability to address a defined problem statement or meet a defined business requirement. Sourcing a purchased service provider involves a range of pricing mechanisms such as fixed price, contingency, rate card, milestone-related, outcome-dependent and many others. Clear scope and statement of work is critical with services, and relationship fit has to be evaluated, while with products contracting you can generally leverage competition.
“While far from ideal, it is much easier to ‘window shop’ when sourcing tangible products than it is with intangible services,” Walsh says. “Suppliers can bring in samples of products, and specifications are readily available, this making comparisons between products relatively straightforward. This is exponentially more challenging to do with intangible services.
Job Aides and Contract Templates
“Master service agreements and purchase agreements have little in common,” Walsh says. We invested the time with our legal team to develop contract templates specific to purchased services. Statements of work are added to master service agreements to simplify the ongoing documentation of additional work with existing service providers.”
Analysis and Planning Strategies
These include establishing a taxonomy for classifying purchased services expenditures, spend analysis – which is ongoing – and gaining access to departmental budgets.
Stakeholder Engagement is Essential
On the product side of the equation, companies often put a procurement policy in place that supply chain must to be involved with every product decision inside the company. However, this approach doesn’t work very well in services. Walsh says that in the multiple companies he’s come from, he’s always found that the better approach is to earn your seat at the table one stakeholder at a time, one project at a time, until they invite you to be there. Otherwise, project engagement is unnecessarily confrontational, awkward and unproductive.
Without earning that seat first, Walsh says, “you’d never have that open dialog with stakeholders where they’re willing to share the salient information required to manage a strong process. They cannot be forced to use you as a service.”
Getting the cross functional team in place, holding kickoff meetings, presenting business justification, listening to and bringing stakeholders along are all very important. With every opportunity initiation, Walsh’s team gathers initial spend data, establishes a schedule, and completes a communication plan.
Intermountain’s highly collaborative process of contracting purchased services doesn’t work if stakeholders lack trust in the procurement process. Walsh’s team has met with relatively little resistance in offering a more structured and measurable procedure for purchasing services and he attributes their success to a focus on relationships and an approach that at its core is all about change management and bringing stakeholders along. The culture of an organization can quickly derail any initiative and each stakeholder has to believe in the value of procurement’s approach.
“You have to prove your worth in each services category by actually demonstrating value in some of the lower-risk areas before stakeholders are willing to give up these relationships that they perceive to have tremendously high value and high risk,” he says.
Checkpoints and Stakeholder Gates
Throughout the process, Procurement is checking back with stakeholders to ensure the need is clearly understood. As implementation gets underway, they touch base regularly to see that the contract and vendor are serving the need.
In each of the six steps in the sourcing/contracting process is a checkpoint that includes as many as a dozen assessments, tests and analyses. Walsh says “we never want to get to the end of the road and then find out that we contracted a statement of work inconsistent with the stakeholder’s needs or requirements. Statements of work are developed with our stakeholders as they are ultimately responsible for the work performed by the contracted service provider.”
Program Management Process
Program management starts post negotiation and involves developing and ensuring program parameters are enforced. Supplier performance is continuously monitored to ensure contract compliance but also to feed learnings back into the process and continuously improve purchasing strategy tactics. With each engagement, procurement and stakeholders are better able to delineate timelines, resources and deliverables. Walsh’s team is regularly involved in stoking stakeholder engagement with frequent dialogs to keep the program current to the evolving needs of the system.
“There are three distinct phases to any contracting process,” Walsh says. “The first phase is the sourcing process, whereby the supplier and the services are selected. The second phase is the contracting process itself. The third phase is the contract lifecycle management phase. This third phase requires comprehensive program management for most purchased services. When contracting tangible products, the contract lifecycle management is a function of price management, transaction management, logistics management, innovation management and other supply-chain centric activities. The contract lifecycle management related to a services contract is dramatically different. If a hospital has a contract with a service provider of cafeteria food services, then a team of hospital representatives must be involved with direction setting, daily operational topics and service issues. The contract governs these terms, but someone must administer the operations. This is not insignificant.”
Step Four in the Journey: Establishing Governance Model and Councils
Walsh’s team set up a procurement governance strategy that includes three different levels of decision-making. A Steering Committee of executives was established to sets priorities for the sourcing team. Fifteen Category Councils were established to review and approve sourcing decisions on behalf of the entire system. These Category Councils collectively cover 100% of the expenses and each have appropriate cross-functional representation and substantially similar rules of engagement. Category Councils report to the Steering Committee, and Sourcing Work teams are established as needed under each Category Council to execute sourcing projects.
“It’s important that we don’t make prioritization decisions without clear direction from our valued stakeholders,” Walsh says. “Additionally, we need to ensure that we help the organization facilitate appropriate debate among cross-functional representatives and every line of business when making important decisions. Leadership and our stakeholders have been overwhelmingly supportive.”
Procurement now has authority to go after 100% of spend with no exceptions. They prioritize projects with senior leaders and work directly with them on decisions and governance.
The Last Step: Metrics
Measuring success in purchased services at Intermountain is dramatically different than it is with products.
Walsh says a common mistake with purchased services metrics is to over rely on process-based measures, rather than focusing on outcome measures. When buyers use process-based metrics, it’s with the usually incorrect assumption that they know exactly what processes are needed to achieve the desired outcomes.
Focus on Outcome Instead of Process
Process measures focus on the steps necessary to accomplish a targeted outcome. Outcome measures focus on the outcome itself. Said another way, the outcome is the lag measure and the processes reflect the lead measures. For internal processes, it is important to measure both as process measures are a reliable predictor of desired outcomes. For example, if your goal is to increase your miles per gallon on your family sedan (the outcome measure), then it would be informative to track process measures such as tire pressure, speed, weight and others.
It is important to recognize that purchased services are about contracting the outcome and you are hiring an expert to manage the processes. When a buying organization overemphasizes the process measures, they are potentially missing the entire point of hiring experts in the first place.
“Companies make this mistake all the time but paradoxically we don’t make this mistake in our personal lives as often,” Walsh says. “For example, when hiring a pest control company for your home, we measure their success by the absence of pests (outcome measure). We don’t try to specify the frequency of treatments or the chemicals used in the treatments (process measures). Why do we try to control every detail of what a commercial service provider does, when they do it and how they do it? Why not focus on outcomes we desire? It’s a bit ignorant and disrespectful to define process measures for a professional engaged to provide a service your company hired out.”
It’s an important concept also for stakeholders to understand, in fact it’s the key takeaway from what Intermountain’s learned from their purchased services journey according to Walsh. It’s a counterintuitive approach because it’s natural to measure the things that are tangible and that can be seen. But with sourcing or negotiating a service, there is no tangible product.
Walsh uses a consulting example. “If you plan to hire a consulting firm to help your system determine where to build a facility in a new market, then it is very important to focus on what you need in order to answer this question (the outcome). In this situation, you are hiring a consulting firm for their recommendation, which will ultimately inform your decision about where to build your new facility. Therefore, it is not important to define the methodology, the source of their data, their approach to research and their validation process. The sourcing process should confirm the consulting firm’s capabilities in these areas of course, but the management of the engagement should focus on the outcome and milestones leading you to the outcome. Resist the temptation to prescriptively tell the consulting firm (or define in granular detail) how to do the work you hired them to do for you.”
Insights and Takeaways
Walsh identifies the shift from a process focus to outcome focus as the key purchased services takeaway – for supply chain as well as stakeholders. In addition to this insight, I’m grateful to Joe for pointing out the importance of having a change management mindset when launching a purchased services initiative. The cultural aspect of making changes in this area requires collaboration, relationship building and an ability to set the stage for everyone being brought along willingly, for the good of the organization. His real-life examples of the “tough conversations” with leadership and stakeholders are great examples of how to effectively make the case and to persuade from a place of knowledge in order to influence change successfully.